
Vertebral Body Tethering (VBT) – Modern Motion-Preserving Correction of Idiopathic Scoliosis

Definition
Idiopathic scoliosis - the most common type of scoliosis where a definite cause is unknown - is a three-dimensional spinal deformity that is associated with:
- a lateral deviation wherein the spine curves sideways abnormally,
- rotation (twisting of the spine) and often with
- a disturbance of the lateral spinal profile.
Classification
Idiopathic scoliosis can be divided according to age into:
- idiopathic infantile scoliosis (development up to the age of 3)
- idiopathic juvenile scoliosis (onset between 4 and 10 years of age) and
- idiopathic adolescent scoliosis (onset from 11 years of age).
Scoliosis can also be simplified into early-onset scoliosis (children younger than 10 years) and late-onset scoliosis (children and adolescents older than 10 years). In children and adolescents with incomplete skeletal growth, there is always a risk of further deterioration of scoliosis. Therefore, this is taken into account during the initial diagnoses and follow-up examinations based on the child’s age.
The severity of a scoliosis is determined radiologically according to the Cobb angle (measures the degree of side-to-side spinal curvature); after precisely locating the main curvature in the thoracic or lumbar spine and also incorporating the lateral spinal profile (kyphosis or normal position), a classification according to Lenke is made. Lenke Classification enables surgeons to communicate about scoliosis based on radiological images in a simple, accurate and consistent way.
Therapy
Therapy of idiopathic scoliosis depends on age, radiological parameters such as scoliosis angle or radiological lateral spine profile measured e.g. according to Cobb, extent of rib hump and lumbar bulge, and skeletal maturity. In addition, the therapy is also drawn according to radiological criteria and the resulting classification according to Lenke.
Conservative therapy with physiotherapy
In the case of a scoliosis angle below 20°, conservative therapy is based on physiotherapeutic exercise treatment,
Conservative therapy with corset (scoliosis brace)
Between a scoliosis angle of 20° to 40° it is treated with physiotherapeutic exercise and corset (scoliosis brace) treatment to straighten out the scoliosis and prevent it from advancing.
Surgical therapy
Surgical therapy is considered for a scoliosis angle greater than 40°, for progressive scoliosis at a growing age, two years after menarche for neurological disorders, or due to limitations of cardiopulmonary function. However, surgical therapy may also be considered for early-onset, severe deformities. In such cases, growth-following or growth-guiding procedures (such as Magec, Reflect, Vertebral Body Tethering) are more likely to be possible. Surgical therapy can be performed by anterior instrumented procedures with rod-screw system, short and long extension, or dorsal procedures (internal fixator with and without lamina hooks and pedicle hooks, etc.).
In practice, it is possible to achieve the greatest possible complete correction (> 80%) of the deformity by dorsal procedures, taking into account a shoulder asymmetry or a rib hump and lumbar bulge. However, a classic corrective spondylodesis involves spinal fusion surgery which is associated with a loss of function in several spinal segments.
The Vertebral Body Tethering (VBT) procedure (implants from Globus Medical, USA, Reflect) is able to successfully treat idiopathic scoliosis by modulating the spine as the child grows while preserving spinal mobility and flexibility. This vertebral body growth modulation technique with a screw-tape system is a novel method that has been clinically tested in the USA for more than 15 years with positive short and long-term results. The method can be performed with specifically approved implants. The first medical device available on the market and specifically approved for this treatment is the ReflectTM screw-band system from Globus Medical.
Picture 1: Illustration of the VBT System Reflect on the spine model

Early-onset spinal deformities have historically had a poor prognosis, not least because of the increased incidence of thoracic insufficiencies. Conservative procedures were often used arbitrarily, and surgical options were limited. Older growth-guiding measures had a high complication rate. Early spinal fusion could not prevent the progression of the vicious circle the children entered in terms of thoracic and pulmonary development to thoracic insufficiency syndrome with increasingly laboured breathing, fatigue, detail disorders, etc. The method of the vertebral body growth modulation technique with a screw-tape system can potentially fulfill this demand of pediatric surgeons for a method not requiring fusion surgery. Thus, the method also has the potential to positively influence not only the clinical complaints of children and the long-term prognosis of the disease, but also the entire psychosocial development, family life, and its division.
Description of the surgical procedure
Preparation of the patient
- Preoperative radiological whole spine radiographs a.p (scoliosis angle and extension and position of the curve) and lateral (lateral spine profile)
- Radiological bending images (statement on rigid and mobile spinal segments).
- Radiographs of the pelvis (Risser classification to calculate growth prognosis).
- Risser classification is used to grade skeletal maturity and estimate the growth potential of an adolescent’s spine.
- X-ray of the left hand (Sanders classification for additional calculation of growth prognosis).
- The Sanders classification offers a reliable estimation of skeletal maturity using a radiograph of the left hand to predict the peak growth phase.
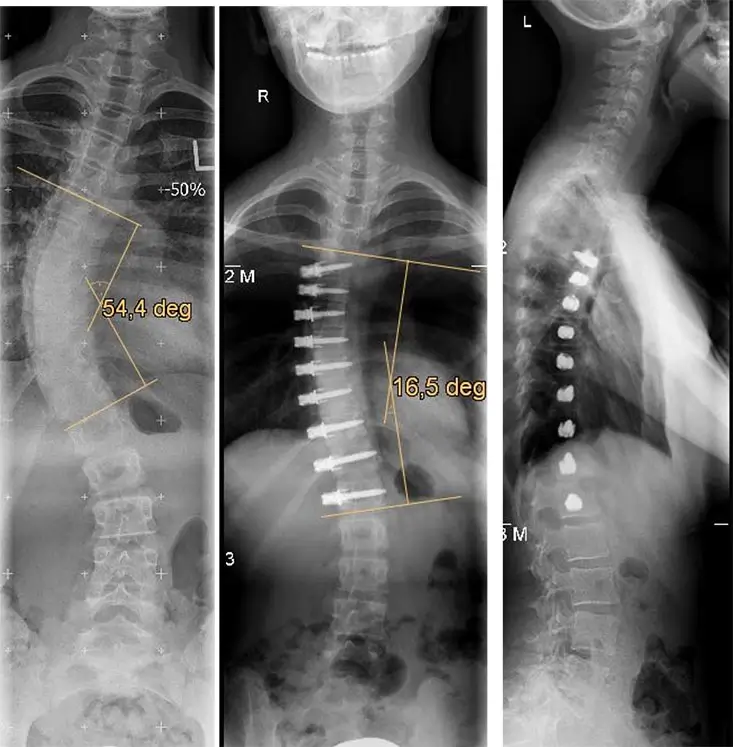
Picture 2: Example of a patient with idiopathic scoliosis, who was treated with the VBT via a minimally invasive approach in the thoracic and lumbar spine. Rontgen image of the entire spine in AP and lateral radiographs before surgery and after VBT surgery.
Surgical technique
Under general anesthesia, small staples are first positioned in the lateral position via minimally invasive approaches in the region of the anterior thoracic spine or the lumbar spine under X-ray control. Screws are then inserted into the vertebral body. Throughout the operation, spinal cord function is monitored using neurophysiological techniques. Starting at the uppermost screw, a cable is fixed and the deformity is gradually straightened from screw to screw using a special tensioning device.

Dr. med. Uwe Vieweg is the chief physician at the department for surgical and conservative spinal therapy, Rummelsberg Hospital, Germany. Dr. Vieweg has enormous expertise in spinal and revision surgery having performed over 8,000 operations of the cervical, thoracic, and lumbar spine. He is also specialized in complex interventions on the spine, especially in previously unsuccessful spine operations, correction of various spinal deformities (kyphosis, scoliosis, spondylolisthesis), minimally invasive microsurgical operations, and disc replacement implantation.
As top healthcare providers in Germany and Europe, Sana Hospitals offer a wide variety of surgical treatment options for pediatric and adult spinal deformities. Our center in Rummelsberg is nationally recognized for the advanced and innovative surgical methods it offers, including Vertebral Body Tethering (VBT).
Featured Blogs

Medically Induced Coma: What It Is, How It Works, Who Benefits, and Recovery Outcomes

